A-scan Technique
Positioning the probe:-
Principle:
Anesthesia
Touch cornea
Positioning the probe:-
Principle:
Anesthesia
Touch cornea
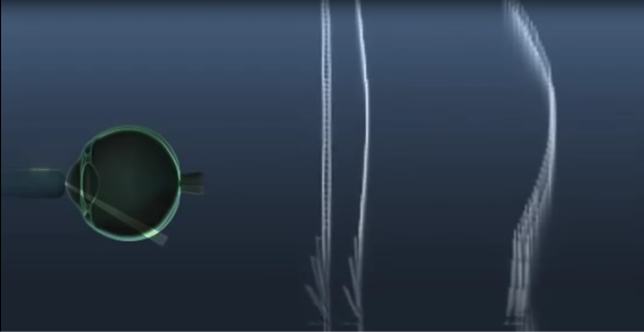
A-scan is a time amplitude. The first structure the sound wave hits is the cornea, thus generating the first spike. Then tow spikes for anterior and posterior len capsules. There is no spike in the normal clear vitreous. And then spikes for the retina and choroid and sclera posteriorly.
Hundred of A scans are aligned together along the posterior retina and then taken at 90 degrees. By joining the dots and 2D B-scan is generated.
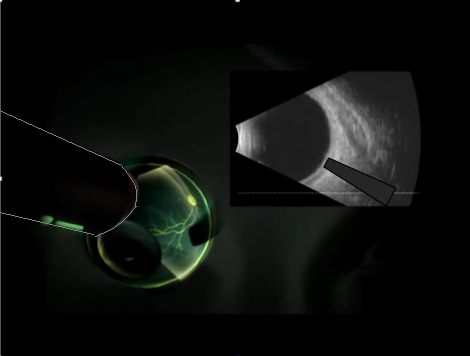
The vector line: represents the one A-scan, at that position, that is displayed at the bottom of the screen.






It represents the one A- scan, in that site, at that position,
that is displayed at the bottom of the screen
The greater the perpendicularity, the more steeply rising the spike is from baseline and the higher the spike.
Positioning the probe:




Anaesthetize eye if using conjunctival approach.
Put Gel.
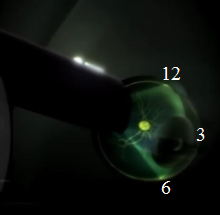
Locate probe mark .
It always represents upper screen.
vTransverse
vLongitudinal
Transverse position
(Parallel) to limbus
Longitudinal position
(Perpendicular) to limbus
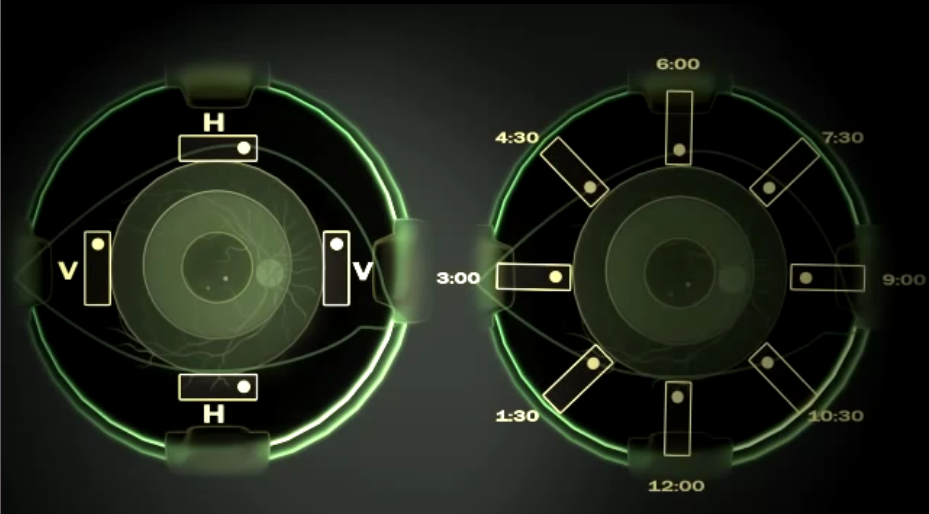
Transverse position (Parallel) to limbus
Mostly used position beside axial scan. Basic screeing.
Right eye. Patient looks down.
Probe in superior limbus.
Mark: nasally, horizontally.
Locate optic nerve.
Scan inferior retina.
Lateral extent of pathology
Repeat for other gazes.
LE (O.N. nasal)
Inferior retin
Transverse position



Patient looks nasal.
Probe in lateral limbus.
Mark pointing superiorly (Vertical position).
Locate optic nerve.
Sweep probe horizontally to see nasal retina.
6 clock hours